Knowledge on PEP among clinical medical students in developing countries is very low calling for inclusion of PEP in HIV curricula.
Continue readingFew Medical Students in Developing Countries Aware of HIV Prevention Drugs
Knowledge on PEP among clinical medical students in developing countries is very low calling for inclusion of PEP in HIV curricula.
Continue reading
Health News: College Campuses receive HIV Awareness from Love Heals Advocates, HIV Progression spotted on Charlie Sheen from Facial Skin Lesions, Recent Progress against Aids Marked in World AIDS Day at Palm Springs
Continue reading
An extremely informative video on the science of HIV and AIDS made by AsapScience on Youtube
Continue reading
Availability of new integrase inhibitors offers better opportunities to improve efficiency of cART and PEP in controlling HIV replication.
Continue reading
In the news -Today reports better Life For Singaporean HIV Patients; Highest cases of HIV in Eastern Europe reported by WHO; The CDC in the US says HIV Prophylaxis can help millions
Continue reading
Truvada® is commonly used in combination with Isentress® for PEP due to the effectiveness and lack of negative interaction between the two drugs. Learn more in this detailed guide.
Continue reading
Overspending, corruption, and tax avoidance seem to have little to do with HIV rates. In 2012, the world watched stunned as Greece’s economy collapsed. Frantic negotiating with the EU seemed to have rescued the failing state, imposing strict austerity measures on the one prosperous nation.
Greece’s unemployment rose to 20%. In the younger demographic it rose as high as 60%. Cuts across the health system led to the abandonment of non-essential health programs, including the reduction to HIV screening of mothers, the clean needle exchange programs. (Kentikelenis et al., Lancet, Volume 383, No. 9918, p748–753, 22 February 2014).
Suicides and drug use rose. The number of women working in prostitution also rose dramatically (Linda Smith, International Business Times, 1st July 2015).
And HIV rates rose 200 fold.
In this first world country, the crisis saw HIV cut a swath through the disadvantaged population. Drug users injected more frequently rather than smoking or snorting as it gave more bang for their buck and without the clean needle program, HIV passed easily from one to the other in shared needles. Refugees, immigrants and married women, all barred from working legally in the Greek sex work system took to the streets and illegal brothels in a desperate attempt to find work. Lacking the protection of the state system they were open to abuse and HIV reared its ugly head once more.
The health care system was no longer able to afford a supply of antiretrovirals to all who needed them, much less post exposure medication to prevent infection like HIV PEP. Doctors had to be selective in who they were able to help. Those who would otherwise live with the inconveniences of a HIV infection found themselves at the mercy of full blown AIDS.
A shocking and scary truth was revealed. HIV, the plague of the 21st century was not under control as we thought. It was being held at bay with a plethora of government strategies, needle exchange programs, education. As soon as these barriers weakened, the plague surged forward to take new ground.
There is some good news to be found though. The low-cost prevention programs, needle exchange, provision of condoms, education, they are all still working hard, despite financial challenges, to stem this tide. If we can take anything from the tragedy of the crisis in Greece it is that the healthcare system, when given sufficient support, can make a huge difference to the spread of HIV. The cost Greece will incur in five or ten years when the AIDS epidemic makes itself known will well and truly eclipse any savings they have made in not buying clean needles. All these small efforts combine to make a huge difference to the health and well-being of the state as a whole and should be recognized for the good work they do.
References:
Kentikelenis et al., “Greece’s health crisis: from austerity to denialism”, Lancet, Volume 383, No. 9918, p748–753, 22 February 2014
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)62291-6/abstract
Linda Smith, “Greek crisis: Thriving sex industry shows austerity has violated women’s rights” International Business Times, 1st July 2015
Isentress® is one of the newest classes of antiretrovirals, the intergrase inhibitors. This drug disables the HIV intergrase protein which is responsible for integrating the viral genome into the human chromosome and causing the chronic incurable infection. Developed by Merck and Co, it was approved for adult use in 2007 by the FDA and use in children as late as 2011. It has been shown to be the most highly effective anti-HIV drug in lowering viral load (numbers of virus in the blood).
Despite the drug’s effectiveness, it does have an Achilles heel. The intergrase protein is highly mutagenic and resistance can develop quickly meaning that Isentress® must be used in combination with other antiretrovirals to be effective. HIV PEP therapy at our clinic includes the use of Isentress® together with Truvada® – a pill made by Gilead Sciences containing Emtricitabine (Emtriva®) and Tenofovir (Viread®). This is currently our preferred PEP treatment combination.
Side effects
Isentress® has fairly mild side effect compared to many other antiretrovirals for most people. It is common to experience insomnia and the resulting tiredness as well as headaches, dizziness and nausea.
Less common side effects are stomach pains, depression including suicidal thoughts, hepatitis, kidney disease and weakness. Help should always be sought immediately if you are experiencing suicidal thoughts and if you start to experience the onset of hepatitis symptoms, most notably jaundice, dark urine, clay coloured stool and loss of appetite. You should be tested regularly for kidney health while taking PEP and it is important that you attend all tests as they will pick up problems before they become bigger. The rebound of hepatitis can happen when treatment stops due to the removal of suppression of HBV by Isentress®. Your doctor should be alerted if you have HBV so that your liver function can be safely monitored following cessation of treatment.
A rare and rather strange side effect of Isentress® is outbreaks of Herpes sores in those who suffer from genital herpes or cold sores and the occasional outbreak of shingles. It is not known what causes this, but is likely to be due to stress on the immune system. Inform your doctor if you suffer from herpes or cold sores or if you have had shingles in the past before starting this medication.
Like any medication, allergies are possible and can in extreme cases be life threatening. Seek emergency medical assistance should you find a rash in combination with fever, extreme tiredness, unexplained muscle or joint pains, sores in the mouth, swelling around the eyes or inside the mouth or difficulty breathing. Do not take any more of the medication if these symptoms appear until given the all clear by your doctor.
Contraindications
As with all PEP drugs, hepatitis or other liver conditions and any kidney conditions need to be closely monitored while taking Isentress®. It has not been shown one way or the other what effects it has on a growing foetus so inform your doctor if you are pregnant and Isentress® should only be taken if essential during pregnancy. There is no indication it is harmful to the baby, but not enough information to say that it isn’t. You should never breastfeed while on PEP, not only because the medication is transmitted through breastmilk but also to prevent transmission of HIV virus that has not been inactivated. PEP is not a cure for HIV, it inhibits the virus long enough for the immune system to respond and it doesn’t always catch it in time. You should behave towards others as if you were infectious until the PEP has been proven to have prevented a chronic infection.
There are indications that Isentress® can exacerbate rhabdomyolysis or myopathy as well as other conditions that increase the levels of creatine kinase in the blood. Inform your doctor if you suffer from any of these conditions and seek advice should you experience any unexplained muscle weakness or pain. As always these are not a full list of the side effects, should you experience anything that concerns you that appears to be linked to starting Isentress® speak to your doctor.
Drug interactions
There are few drugs that have a risk of negative interactions with Isentress®. One to watch for is Magnesium supplements. The magnesium or aluminium in these supplements can bind to the Isentress® and inactivate the drug. You should stop taking multi-vitamins or antacids when starting Isentress® treatment as many of these contain magnesium and/or aluminium.
There is some indication that the antibiotic rifampin may speed up the liver in clearing Isentress® from the body. You should try to ensure that you attend the same doctor while on PEP so that he or she is aware of all the medications you are taking. If you do need to see a different doctor make sure they are aware you are taking PEP. It may be that the doctor will have to change the prescribed dose of Isentress® while you are taking rifampin to ensure the levels are sufficient to inactivate any HIV virus.
Other drugs to watch for are any others that increase liver metabolism or those that raise the acidity of the blood, both may decrease the effectiveness of Isentress® and the active levels will need to be monitored while on these drugs. It will inevitably mean more blood tests, but despite the inconvenience, it is better to have a host of blood tests over the 28 days of treatment than have to have constant blood tests for the rest of your life because a HIV virus slipped past the drugs and integrated.
You should advise your doctor of any herbal remedies or supplements you are taking before starting any medication. As Isentress® is a relatively new drug it is likely there are other drugs it will react with in a negative way that are not yet known. If you feel unwell after taking another medication in combination with Isentress® inform your doctor immediately. If that medication is non-essential stop taking it immediately. If it is essential seek urgent medical advice regarding how to proceed.
Additional information
As Isentress® has only been approved for human use for less than ten years there is still a good deal to learn about how exactly it acts on the virus. Studies have shown surprising results with Isentress® notably that while the intergrase was thought to only cause integration into the human genome, blocking it resulted in viral loads falling faster with Isentress® than with the nucleoside reverse transcriptase inhibitors or the protease inhibitors. As both of these alternatives directly impact on viral replication, it would suggest that the intergrase has a more essential role in HIV replication that previously thought.
Work on other viruses, notably Hepatitis B (HBV) and Epstin-Barr virus have shown that despite being designed for HIV, Isentress® may be effective against a much wider range of viruses. Like Viread, Isentress® can cause a rebound effect in HBV sufferers as it is believed to lower HBV loads which recover when PEP treatment is stopped causing a bout of acute hepatitis. While not approved for treatment of HBV there are clinical trials currently assessing its effectiveness against HBV and it may offer hope in future for HBV sufferers.
Epstine-Barr virus (EBV) is a member of the Herpesviridae family (Lymphcrytovirus Human herpesvirus 4) and causes glandular fever (also known as infectious mononucleosis, mono or the kissing disease). It is one of the most common viruses and as well as being known for causing post-viral chronic fatigue, it is less well known as a risk factor in various cancers, notably gastric cancer and a variety of blood cancers (lymphoma) and autoimmune diseases such as lupus, rheumatoid arthritis and multiple sclerosis. Preliminary clinical trials with Isentress® suggest that the drug may be successful in reducing the severity of EBV-associated multiple sclerosis. If trials prove successful, it will lead to a very exciting possibility of treatment for this horrific disease, and perhaps many others.
It is a wonderful example of cross-discipline drug development where eagle-eyed doctors noticed a correlation between use of a drug for one purpose and followed through with their observations. The result of which is a HIV drug that not only provides hope for those with HIV, but spreads out to potentially treat cancer and autoimmune disease as well.
Watch this space, very exciting developments going on.
For more information see:
WebMD – Isentress®
http://www.webmd.com/drugs/2/drug-149324-1036/isentress-oral/raltegravir-oral/details
Isentress® product information.
https://www.isentress.com/raltegravir/isentress/consumer/hiv_medication/
Information on use of Isentress® in treatment of relapsing Multiple Sclerosis
Research has played a vital role in changing the face of the medical field. From untreatable diseases to highly contagious diseases, research made wondrous achievements and solved the previously unsolvable. The research on HIV has also provided us with life-saving treatments like a prophylaxis from HIV. The WHO (World Health Organization) convened a meeting in June 2014 to develop guidelines for the use of HIV post-exposure prophylaxis (PEP). During this meeting, gaps in research were also uncovered. This paper published in Clinical Infectious Diseases® reports the background, methodology, results and conclusions of a study to create a framework for future research.
The Grading of Assessment, Evidence, Development and Evaluation (GRADE) system and clinical management pathway were used for formulating the research questions required for future research. The study reported and analyzed current WHO recommendations for HIV PEP and graded its quality of evidence as well. The recommendations were formulated with the help of the Guideline Development Group (GDG) created by the WHO.
For the study, a clinical management pathway for HIV PEP was made which included the following steps:
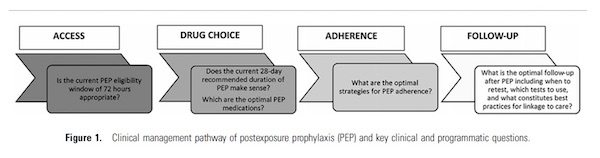
The formulated questions for each of the above mentioned clinical management pathway stage were thoroughly searched from current WHO guidelines and other online databases. The available data was collected, the gaps were identified and the GDG (Guidelines Development Group) helped the authors formulate future recommendations for each step.
Surprisingly, the study shows that the available guidelines of the WHO on the HIV PEP are mostly based on low-quality of evidence. Many of the clinical management questions that were formulated at the start of the study had no available study or recommendations.
On the whole, three study design formats for the future research were identified in the study which included the survey and interview driven research for identification of barriers related to PEP. Second was the establishment of a PEP registry on a global scale for drug choices, usage details, follow-ups and toxicities in specific drug regimen for PEP. Thirdly, randomized control trials for determination of the most authenticated evidence related to PEP.
For the study of access to PEP, the report suggests conducting cross sectional studies. To study the timing and duration of PEP, the recommendations are to have randomized control trials. These trials are also recommended for the study of the drug choice, adherence to the drug and the follow-up. Randomized control trials are lacking in comparing the HIV PEP drugs at different ages, hence the report recommends randomized control trials in it too.
The interesting thing reported in the study was that there is no future research needed in regard to the question whether a 28-day regimen for PEP is appropriate. The report mentioned that a 28 day PEP regimen is most appropriate and this recommendation does not need any future studies.
A 3-day movement was started in Mumbai, India, to spread awareness of the use of HIV PEP as a preventive measure for rape victims from getting infected by the HIV virus. Several medical professionals and institutions took part in this movement. Although it is an established fact that the chances of a rape victim being infected by the virus is extremely low when treated within 8 hours of exposure, the treatment is not provided or mandated at a national level in India. This is what this movement is trying to change.
Dr Ishwar Gilada, who is the president of the AIDS society of India, was reported as claiming to the press in India that if a rape victim is given PEP treatment immediately, chances of infection can go down to as much as 100%. This movement comes after the recent rise in rape incidents in India. There were a reported 36735 rape cases in 2014 – statistics given by the National Crime Records Bureau (NCRB) statistics. Gilda said that HIV PEP therapy should be prescribed in addition to trauma care. The initiative to request for this medication should be made by both the relatives of the victims as well as law enforcement.
Read the full report here: http://www.uniindia.com/post-exposure-prophylaxis-can-prevent-hiv-infection-if-administered-within-8-hours-dr-gilada/others/news/254245.html
A study was made in London on the drug usage and sexual patterns on men who have sex with men. They study was made on 874 male participants who used the services of a chemsex support service provided by the busiest STD Clinic in London, the 56 Dean Street clinic. Chemsex is the act of using a variety of recreational and, mostly illegal, drugs to remove any sexual inhibitions as well as increase arousal and desire, resulting in periods of sexual intercourse that may last for days. One of the more popular drugs used is crystal meth.
Data collected from the survey revealed that 70% of the men who attended the clinic used drugs in all their sexual activities during the last six months. They had no recollection whatsoever of what sober sex feels like anymore. This shows a worrying dependency on drugs by these individuals for sex. In the group of men being studied, 32% of them were HIV positive, out of which 42 of them were not being treated with antiretroviral therapy and 64% of them did not use condoms during sexual activities.
For the remaining HIV-negative men, forty percent used condoms less than half the time and ten percent reported no use at all. 30% of these men were medicated with HIV PEP once at least during the last 2 years while 25% had taken the medication up to 10 times. Interest in PrEP treatment in this group of men who engage in chemsex is extremely high while a third of them do not that know such a treatment exist.
For the full report go here – http://www.aidsmap.com/London-clinic-survey-shows-impact-of-chemsex-on-condom-and-PEP-use/page/3009821/